<i>Supervised detection of newly appearing T2-w multiple sclerosis lesions with subtraction and deformation fields features
</i>
Research Abstract
Background: MRI has become one of the most important clinical tools for longitudinal analysis of multiple sclerosis (MS). Newly appearing lesions are indicative of the disease progression. Several automatic approaches have been proposed for the detection of newly appearing lesions, which can be classified as either supervised approaches that use intensity-derived features from the subtraction images or unsupervised approaches that use also deformation fields information.
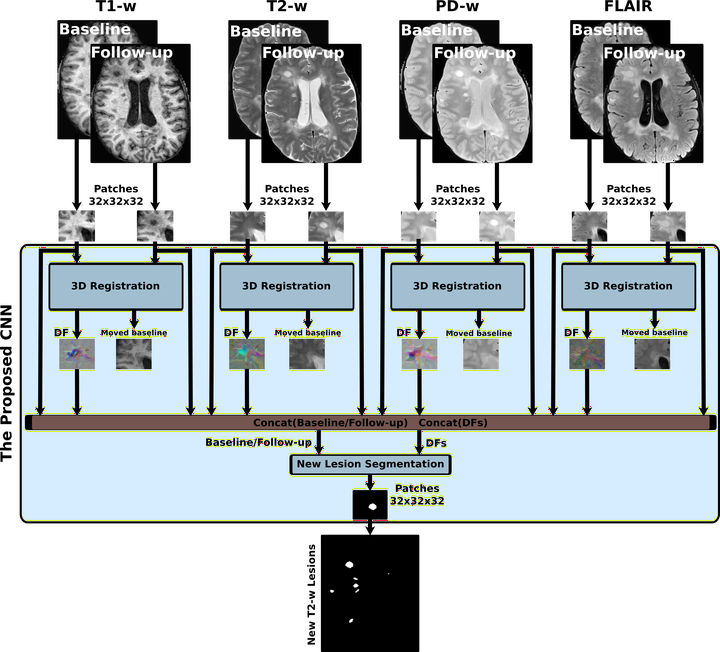
Aim: We present here a supervised approach for detecting newly appearing MS lesions that combines both subtraction and deformation field features. Specifically, we use a logistic regression classifier trained with features from the baseline and follow-up intensities, subtraction values, and deformation field operators to provide a final segmentation.
Materials and methods: One year apart multi-channel brain MRI were scanned for 60 patients with a 3T magnet, including transverse T2-FLAIR, PD-w, T2-w and T1-w images. 36 of these patients presented new T2-w lesions that were semi-automatically annotated by expert neuroradiologists. The rest had no new lesions in the follow-up scans. All images were pre-processed and co-registered by multi resolution-multi stage affine registration, and a deformation field was also obtained using the Demons non-rigid registration algorithm.
Results: We performed a leave-one-out cross-validation strategy using the 36 patients with new T2-w lesions. In terms of detection, we obtained a 74.30% true positive fraction and 11.86% false positive fraction with a mean Dice similarity coefficient of 0.77. In terms of segmentation, we obtained a mean Dice coefficient of 0.56. We compared these results with those obtained with state-of-the-art methods such as Sweeney et al. (2013), Ganiler et al. (2014), and Cabezas et al. (2016), and our model had significantly better results (p 0.05). When testing the model with the 24 patients with no new T2-w lesions, only 5 false positives were found in 4 cases.
Conclusions: The proposed model decreases the number of false positives while increasing the number of true positives. The study also proves the benefits of using deformation field operators as features to train a supervised learning model. Our approach is simple and fully automated and reduces user interaction and inter- and intra-observer variability.
Disclosure:
M. Salem: nothing to disclose.
M. Cabezas: nothing to disclose.
S. Valverde: nothing to disclose.
D. Pareto: has received speaking honoraria fron Novartis and Biogen.
A. Oliver: nothing to disclose.
J. Salvi: nothing to disclose.
A. Rovira serves on scientific advisory boards for Biogen Idec, Novartis, Sanofi-Genzyme, and OLEA Medical, has received speaker honoraria from Bayer, Sanofi-Genzyme, Bracco, Merck-Serono, Teva Pharmaceutical Industries Ltd, Novartis and Biogen Idec, and has research agreements with Siemens.
X. Lladó: nothing to disclose.
Research Department
Research Journal
Multiple Sclerosis Journal - ECTRIMS (JCR CN IF:5.649 Q1(23/199)), Paris. France
Research Member
Research Pages
pp. 794-794
Research Publisher
SAGE PUBLICATIONS LTD
Research Rank
3
Research Vol
Vol. 23
Research Website
NULL
Research Year
2017